
How to use this patient guide
This guide is intended to help you prepare questions and understand practical directory information. It does not replace advice from your doctor, referrer, clinic, insurer, ACC, or Health New Zealand service. Confirm any instructions, preparation steps, timing, and costs with the clinic before your appointment.
Radiologists are a central part of cancer care in New Zealand’s multidisciplinary teams (MDTs). These teams, consisting of specialists like surgeons, oncologists, pathologists, and others, work together to create tailored treatment plans for patients. Radiologists contribute by interpreting imaging, performing procedures like biopsies, and offering real-time insights during case discussions. Their input helps refine diagnoses, adjust staging, and optimise treatment strategies.
Key Points:
- Radiologists provide imaging insights that guide critical decisions.
- They perform image-guided procedures, reducing the need for surgery.
- MDT discussions, supported by radiologists, can change diagnoses or treatment plans in up to 38% of cases.
- Collaboration with other specialists, like pathologists, enhances diagnostic accuracy.
Radiologists’ expertise ensures that MDTs deliver precise, patient-focused cancer care, supported by national standards and advanced imaging technologies.
The Importance of Multidisciplinary Tumor Boards
sbb-itb-16a0ccc
1. Radiologists
Radiologists play a critical role in multidisciplinary teams (MDTs), turning X-rays, CT scans, MRIs, and ultrasounds into actionable clinical insights that go far beyond simply writing reports.
During MDT meetings, radiologists offer real-time input as surgeons and oncologists ask specific questions and review images live. They clarify details like tumour location, vascular involvement, and lymph node status, making the diagnostic process more precise and improving treatment plans. As Ajith John and Rohin Mittal from the Department of Surgery at Christian Medical College and Hospital point out:
"The smooth steering of MDT relies on an experienced radiologist who helps in staging the disease and offers additional inputs and clarification for interpreting the radiologic images."
A study on oesophago-gastric cancers highlighted the importance of MDT reviews, showing that these discussions led to differing findings in 38% of patients. This included changes to disease staging (21%), diagnosis (9%), and clinical decisions in 26% of cases. Notably, treatment plans shifted from palliative to curative in about 9% of patients.
Beyond image interpretation, radiologists also perform interventional procedures like image-guided biopsies, drainages, and catheter insertions, which can sometimes replace the need for open surgeries. In New Zealand’s BreastScreen Aotearoa programme, radiologists work closely with surgeons, pathologists, and breast care nurses, showcasing their expertise in ultrasound and minimally invasive diagnostics.
Their contributions to MDTs can be grouped into four main areas:
| Responsibility | What It Involves |
|---|---|
| Diagnostic | Interpreting imaging results and providing differential diagnoses |
| Procedural | Carrying out image-guided biopsies, drainages, and catheter insertions |
| Consultative | Advising on imaging needs, reviewing complex cases, and recommending modalities |
| Safety & Quality | Overseeing radiation safety, conducting peer reviews, and ensuring procedural standards |
These diverse responsibilities highlight the essential role radiologists play in MDTs, laying the groundwork for comparisons with other specialists’ contributions.
2. Surgeons and Oncologists
Surgeons and oncologists play a critical role in transforming imaging insights from radiologists into actionable treatment plans. Surgeons, for instance, assess whether a tumour can be surgically removed by mapping out its anatomical boundaries. This helps them decide on the most appropriate surgical approach, such as a lumpectomy versus a mastectomy. On the other hand, oncologists rely on imaging to guide systemic therapies and monitor how well treatments are working, using tools like RECIST 1.1 criteria.
Surgeons bring an added layer of understanding by combining physical examinations and patient histories with imaging reviews. Associate Professor Ahmad Aly highlights this collaboration, stating:
"The interaction between radiologist and clinicians often results in the focus of certain disease features that alter the stage or treatment intent."
This teamwork is evident in multidisciplinary team (MDT) meetings. A study involving 34 patients with oesophago-gastric cancer found that MDT discussions significantly impacted clinical decisions in 26% of cases. For example, one patient initially diagnosed with a gastric gastrointestinal stromal tumour was later found to have a small bowel tumour after the MDT review. This adjustment allowed for a targeted surgical procedure, even with the patient’s high-risk health conditions.
Surgeons often lead these MDT discussions, speaking for 47% of the time during case reviews. Their input is crucial in revisiting and refining imaging results, which can directly improve patient care.
Oncologists, meanwhile, rely heavily on accurate radiology reports. In fact, 40% of oncologists remeasure tumour sizes one to three times a week due to inconsistencies in the original measurements. This highlights the importance of close collaboration between radiologists and oncologists in MDTs to ensure precise and effective clinical decisions.
3. Pathologists
Pathologists take the diagnostic process a step further by examining tissue samples under a microscope, offering insights that go beyond what radiologists and surgeons can see. While radiologists pinpoint a tumour’s location and surgeons describe its appearance, pathologists determine its biological nature, providing crucial details that guide the multidisciplinary team’s (MDT) treatment decisions.
As researchers Julie E.M. Swillens et al. put it:
"In MDT meetings, diagnostic information is mainly provided by pathologists and radiologists."
Pathologists contribute vital information about tumour type, grade, and molecular characteristics, which helps determine if additional therapies are necessary. This complements the radiologist’s focus on anatomy with the biological details needed for a more complete picture.
The collaboration between pathologists and radiologists is particularly valuable when cases are unclear. For instance, a 2016 study at Austin Hospital in Melbourne highlighted a case where imaging suggested a biliary obstruction, raising suspicion of gastric lymphoma. However, the diagnosis was only confirmed after a tissue biopsy and pathology review. This kind of teamwork in MDT discussions led to diagnostic changes for 9% of patients and adjustments to disease staging for 21%.
Pathologists also play a key role during MDT meetings by providing real-time feedback, which enhances the confidence of their radiology colleagues. Research from the University of Sydney supports this, stating:
"Radiologists believed their confidence in their clinical decision making increased when there was immediate feedback from pathologists."
This dynamic exchange between imaging and pathology strengthens the MDT’s overall diagnostic precision.
To make their contributions even more impactful, pathologists can use Standardised Structured Reporting (SSR). This approach is gaining traction, with 84% of MDT members advocating for more consistent use of SSR and 88% noting that it has already improved pathology reports. The benefits are clear: in colorectal cancer cases, standardised pathology reporting has been linked to improved survival rates, rising from 62.4% to 65.0%.
4. General Practitioners and Allied Health Professionals
General practitioners (GPs) and allied health professionals play a crucial role in kick-starting and maintaining the diagnostic process, working alongside radiologists and pathologists. Their expanded responsibilities ensure that the entire care pathway runs smoothly, complementing the imaging expertise of radiologists.
In New Zealand, GPs, urgent care doctors, and nurse practitioners now have the ability to directly refer patients for imaging. This change allows for earlier diagnosis and treatment, supported by a $30 million annual investment from the New Zealand Government into a community-referred radiology programme, which is expected to be fully operational by July 2026. To ensure referrals are effective, regional hubs staffed by primary care liaison officers evaluate requests using national clinical criteria. These criteria have been developed collaboratively by primary care clinicians and radiologists, helping to ensure radiology resources are directed where they are most needed. Te Whatu Ora highlights the value of this approach:
"Diagnostic imaging helps community and primary care providers to make better decisions about where to refer patients next, or if they can provide care closer to home."
Allied health professionals, particularly radiographers (Medical Imaging Technologists), also contribute significantly through Preliminary Image Evaluation (PIE). In emergency departments, PIE-trained radiographers provide rapid, initial interpretations that support acute care decisions. Their expertise acts as a safety net for junior doctors and nurse practitioners. Ryan Walklin, a radiologist at Taranaki Base Hospital, emphasises their impact:
"The interpretive performance of radiographers can approach and in some cases surpass radiologists… treatment is [otherwise] guided by an interpretation that has significantly lower accuracy than a PIE-trained radiographer."
Digital integration further enhances this collaborative effort. Community referrers can access both current and historical imaging in real time, minimising unnecessary repeat tests and improving clarity in patient care. By leveraging digital records, GPs and allied health professionals strengthen their alignment with the multidisciplinary team’s focus on coordinated, patient-centred care.
Pros and Cons of Each MDT Role
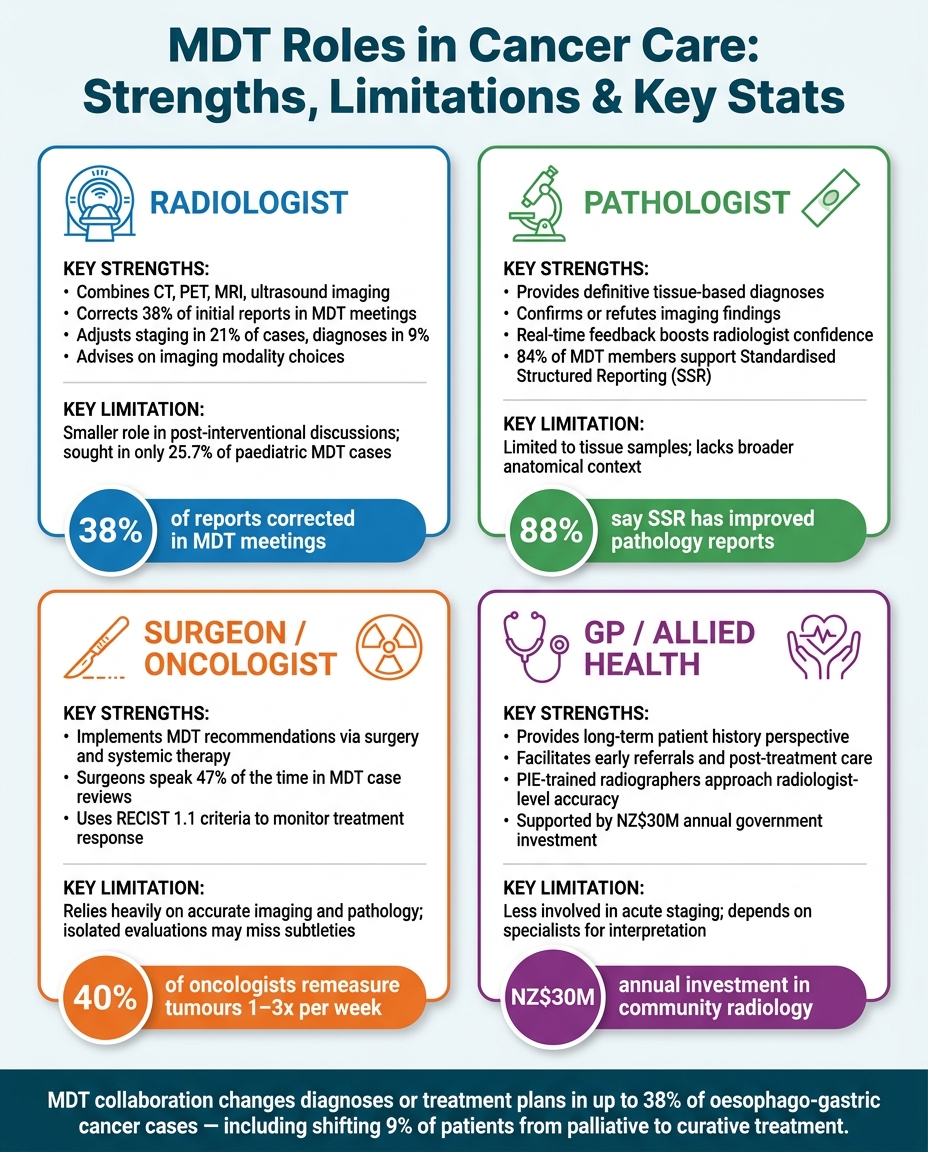
MDT Roles in Cancer Care: Strengths, Limitations & Key Stats
Every member of a multidisciplinary team (MDT) brings a unique set of skills to the table, but no role is without its limitations. This section breaks down the contributions and challenges associated with each role, providing a clearer picture of how they function within the team dynamic.
Radiologists play a key role by integrating various imaging modalities like CT, PET, MRI, and ultrasound. Their ability to refine initial reports is noteworthy – 38% of initial reports in oesophago-gastric MDT meetings were corrected, with staging adjusted in 21% of cases and diagnoses in 9%. Glyn Llewellyn-Jones from The Prince of Wales Hospital highlights their impact:
"Radiologists influence clinical patient management during multidisciplinary team meetings primarily by providing differential diagnoses and guidance regarding future imaging, with respect to both the necessity and the modality."
However, their role is less prominent in post-interventional discussions. For instance, in paediatric MDT cases, specific radiological advice was sought in only 25.7% of instances, though it influenced management in 17.9%.
Other MDT members complement the radiologist’s contributions in their own ways. Here’s a summary of the strengths and limitations of the four key MDT roles:
| MDT Role | Key Strengths | Potential Limitations |
|---|---|---|
| Radiologist | Combines multi-modality imaging; identifies reporting errors; advises on imaging choices | Plays a smaller role in post-interventional discussions; sometimes underutilised |
| Pathologist | Offers definitive tissue diagnoses; confirms or refutes imaging findings | Limited to tissue samples, lacking broader anatomical insights |
| Surgeon / Oncologist | Implements MDT recommendations through interventions and treatments; provides clinical context | Relies heavily on accurate imaging and pathology; isolated evaluations may overlook subtleties |
| GP / Allied Health | Brings a long-term perspective of the patient’s history; facilitates post-treatment care and early referrals | Less involved in acute staging; depends on specialist expertise for interpretation |
Collaboration between roles significantly enhances outcomes. For example, immediate histological feedback from pathologists can boost radiologists’ confidence and decision-making accuracy. Sarah Lewis from the Medical Imaging Optimisation and Perception Group at the University of Sydney emphasises this point:
"Radiologists believed their confidence in their clinical decision making increased when there was immediate feedback from pathologists."
This synergy across roles highlights the strength of MDTs in delivering superior care – achievements that would be difficult to match through isolated efforts.
Conclusion
Radiologists play a crucial role in healthcare, acting as diagnostic experts within multidisciplinary teams (MDTs). They don’t just interpret images; they also perform minimally invasive procedures, bridging the gap between identifying medical issues and treating them. This dual responsibility makes them an essential part of effective patient care.
In New Zealand, structured programmes highlight the importance of this integrated role. For example, BreastScreen Aotearoa brings radiologists together with surgeons, pathologists, and breast care nurses to provide high-quality screening and assessments, showcasing their precision and teamwork.
The move toward remote reporting and subspecialisation in fields like interventional oncology and neuroradiology allows radiologists to support MDTs across multiple regions. This development is especially important as the healthcare system faces workforce challenges. It reinforces the role of radiologists as key collaborators in delivering top-tier cancer care throughout New Zealand.
For those looking for specialist imaging services, Radiology Clinics NZ offers a convenient directory of radiology and imaging facilities nationwide. It helps patients and healthcare providers find the right clinic based on location and service needs.
FAQs
What actually happens in an MDT meeting?
A multidisciplinary team (MDT) meeting brings together specialists such as radiologists, surgeons, and oncologists to discuss and decide on the best care approach for a patient. Ahead of the meeting, the team examines clinical details, imaging results, and cultural considerations. During the session, a chairperson guides the conversation, while radiologists provide critical interpretations of imaging findings, which can heavily influence both diagnoses and treatment strategies.
How can a radiologist change my diagnosis or cancer stage?
Radiologists play a crucial role in cancer care, leveraging advanced imaging technologies such as CT and PET-CT scans to pinpoint tumour locations and evaluate their activity. Their expertise, combined with discussions in multidisciplinary team meetings, often sharpens diagnoses and refines cancer staging. In fact, research indicates that second-opinion reviews by radiologists can change cancer staging in more than 50% of cases, ultimately improving treatment strategies. Radiology Clinics NZ connects patients with imaging services, offering support close to home.
When is an image-guided biopsy used instead of surgery?
An image-guided biopsy offers a less invasive way to collect tissue samples compared to traditional open surgery. By relying on imaging tools such as ultrasound, X-ray, CT scans, or MRI, radiologists can accurately pinpoint and sample abnormal areas. This approach is particularly useful for detecting and targeting small or hard-to-reach issues. It comes with several advantages, including reduced risks, shorter recovery times, and a lower chance of scarring or deformities. At the same time, it delivers the precise diagnosis needed to plan effective treatment.
Related Blog Posts
- How to Read and Understand Your Radiology Report
- Top Clinics Offering High-Resolution Imaging in NZ
- Top PET Scan Clinics in NZ
- Study: AI Impact on Radiology in NZ

Author: Dr. Mark Bekhit
Radiologist and reviewer for Radiology Clinics NZ medical-adjacent directory and guide content.
Sources, method, and medical context
This article is published by Radiology Clinics NZ and reviewed for medical-adjacent accuracy by Dr. Mark Bekhit, radiologist. It is general information only and does not replace advice from your own doctor, referrer, clinic, insurer, or Health New Zealand service.
Official references
- Health New Zealand: scans and X-rays
- Health New Zealand: community-referred radiology service
- Radiology Clinics NZ: how the directory is built
Related directory pages
Radiology clinics directoryBrowse by scan typeBrowse by cityHow this directory is built
Last editorial review: 2026-06-30.
Leave a Reply