
Radiation dose optimisation is about using the lowest radiation necessary to produce clear, diagnostic-quality medical images. This ensures safety while avoiding the risks of overexposure or poor-quality scans. The key is balancing minimal radiation exposure with accuracy, guided by the ALARA principle (As Low As Reasonably Achievable).
Key points:
- Why it matters: Excessive radiation exposure can lead to long-term risks like cancer, especially in children.
- Metrics used: CTDIvol, DLP, and effective dose (measured in mSv) help monitor and manage radiation levels.
- New Zealand practices: Facilities follow international safety standards, including Diagnostic Reference Levels (DRLs), and use advanced technologies to minimise exposure.
- Modern solutions: Iterative Reconstruction (IR) and Deep Learning Reconstruction (DLR) techniques allow significant dose reductions without compromising image quality.
Facilities in New Zealand are adopting advanced imaging tools, dose monitoring systems, and tailored protocols to ensure patient safety. Before your next scan, ask about dose-efficient practices and technologies to minimise your exposure.
Radiation Dose Reduction in CT – Lifeng Yu, PhD
sbb-itb-16a0ccc
Traditional Dose Reduction Methods
Traditional methods for reducing radiation doses have long been a cornerstone of balancing safety with image quality. Before the advent of modern reconstruction algorithms, radiologists in New Zealand relied on manually adjusting scanner settings to manage radiation exposure. However, these approaches often came with compromises, particularly between lowering the dose and maintaining diagnostic image clarity.
Modifying Scanner Settings
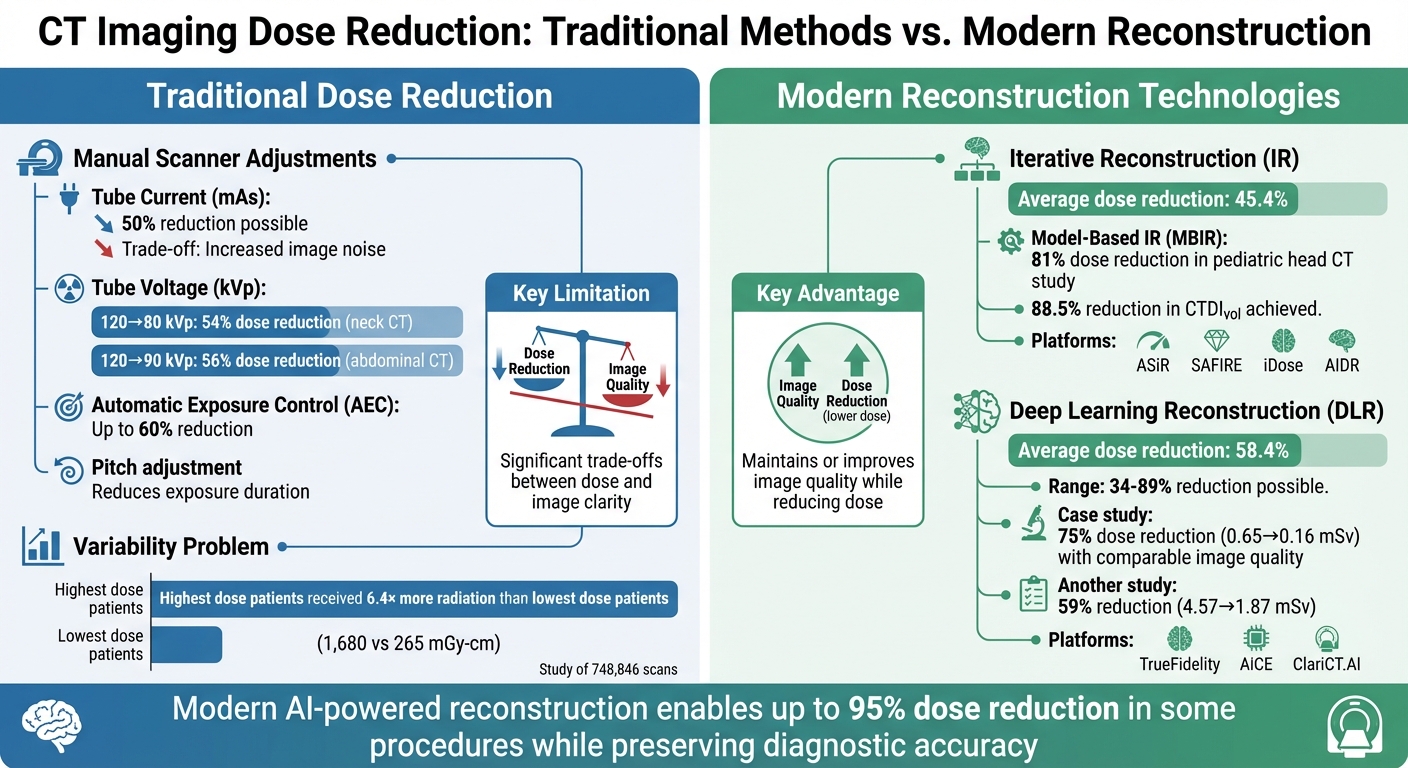
One of the primary strategies involved adjusting the tube current (mAs) and tube voltage (kVp). For example, halving the tube current could reduce radiation exposure by 50%, but this also increased image noise, following an inverse relationship with the square root of the mAs.
Adjusting the tube voltage offered even greater reductions. For instance, lowering kVp from 120 to 80 could cut radiation by 54% in neck CT angiography, while a reduction from 120 to 90 kVp achieved a 56% dose reduction in abdominal CT scans. This method was particularly effective for iodine-enhanced scans, as lower-energy photons interact more efficiently with iodine, enhancing contrast. For patients under 80 kg, reducing abdominal CT settings from 120 to 90 kVp was often achievable without compromising diagnostic accuracy.
Other adjustments included limiting scan length to the required anatomical area, which directly reduced exposure. Automatic exposure control (AEC), a system that dynamically adjusts tube current based on patient size and anatomy, could achieve dose reductions of up to 60% in non-contrast brain CT scans. Increasing the pitch in helical CT scans also reduced the duration of tissue exposure, although it came with a slight decrease in spatial resolution.
Limitations of Traditional Approaches
The trade-off between dose reduction and image quality was the central challenge of these traditional methods. As Lifeng Yu from the Mayo Clinic noted:
"The goal of dose reduction can be approached from… appropriately defining the target image quality for each specific diagnostic task, not requiring lower noise or higher spatial resolution than necessary".
Excessive dose reductions often led to quantum noise, which could obscure low-contrast lesions in critical areas like the liver or brain. In extreme cases, particularly with larger patients, the signal could drop below electronic noise levels, creating severe artefacts and rendering images unusable. Additionally, while narrower beam collimation could improve spatial resolution, it sometimes increased the weighted CT dose index by up to 55% in head phantoms due to overbeaming.
Despite the availability of optimisation tools, their inconsistent application has been a concern. A large-scale study of 748,846 routine abdomen CT scans (conducted between January 2015 and October 2020) revealed significant variability: patients in the highest dose decile received 6.4 times the average dose compared to those in the lowest decile (1,680 vs 265 mGy-cm), even when their body diameters were similar. This highlights the potential for unnecessarily high exposures when traditional methods are not carefully implemented.
Modern reconstruction techniques have since emerged to address these challenges, offering a way to reduce doses without compromising image quality.
Modern Image Reconstruction Methods
Traditional vs Modern CT Dose Reduction Methods: Effectiveness Comparison
Advancements in reconstruction technologies have significantly transformed medical imaging by enabling reduced radiation doses without compromising image quality. Unlike older methods that forced a trade-off between exposure and clarity, these modern approaches use advanced algorithms to minimise image noise after the scan. This allows clinicians to lower parameters like tube current or voltage while maintaining diagnostic accuracy. These developments align with New Zealand’s focus on balancing image clarity and patient safety.
Iterative Reconstruction Algorithms
Iterative reconstruction (IR) methods refine images by repeatedly adjusting estimated reconstructions against measured projections. This process reduces noise and artefacts, addressing the drawbacks of traditional Filtered Back Projection. Studies show that IR can cut radiation doses by around 45.4%. Among these, Model-Based Iterative Reconstruction (MBIR) – often called "pure" IR – delivers even better noise reduction and spatial resolution compared to hybrid IR techniques.
For instance, a pilot study conducted at the Post Graduate Institute of Medical Education & Research in India examined 88 children (ages 5–16) undergoing head CTs for seizures. Using MBIR, the study achieved an 81% reduction in mean effective dose and an 88.5% drop in CTDIvol, all while maintaining diagnostic reliability.
Current IR technologies available include platforms like ASiR and ASiR-V (GE Healthcare), SAFIRE (Siemens Healthineers), iDose and IMR (Philips Healthcare), and AIDR (Canon Medical Systems). However, as Moorin et al. highlighted in PLOS One:
"Fully realising the potential dose reduction of iterative reconstruction requires the adjustment of image factors and forgoing the noise reduction potential of the iterative algorithm".
Building on the success of IR, deep learning reconstruction takes these efforts even further by leveraging artificial intelligence.
Deep Learning Reconstruction
Deep learning reconstruction (DLR) builds on the iterative methods by employing neural networks trained on high-quality imaging data. These networks are designed to suppress noise more effectively, enabling the use of "ultra-low dose" protocols. DLR has demonstrated dose reductions averaging 58.4%, with some protocols showing reductions between 34% and 89%.
A September 2023 study at Seoul National University Hospital compared DLR and IR techniques in 100 patients undergoing CT scans. Quarter-dose (QLD) images (0.16 mSv) reconstructed with ClariCT.AI – a vendor-neutral DLR software – were evaluated against standard low-dose (LD) images (0.65 mSv) reconstructed using ADMIRE, an IR method. The findings revealed that the 75% dose-reduced DLR images delivered comparable nodule detection and image quality to the standard protocol.
DLR also tackles the slower processing times often associated with advanced IR models by using pre-trained neural networks, which significantly speed up image reconstruction. In New Zealand, DLR platforms like TrueFidelity (GE Healthcare), AiCE (Canon Medical Systems), Precis DL, and ClariCT.AI are now widely available.
Another study conducted between May and July 2024 at Wonju Severance Christian Hospital compared reduced-dose abdominopelvic CT scans using a SilverBeam filter with DLR against standard-dose CT with IR. The DLR protocol achieved a 59% reduction in effective dose (1.87 mSv versus 4.57 mSv) while maintaining comparable image quality.
As summarised in a systematic review from Applied Sciences:
"Deep learning reconstruction consistently allowed greater dose reduction than conventional IR while maintaining or improving image quality, as supported by marked noise suppression and enhanced SNR/CNR performance".
Dose Monitoring and Management Systems
While advanced image reconstruction techniques help minimise radiation exposure, it’s equally important to have reliable dose monitoring systems in place to ensure patient safety remains a priority.
Modern dose management platforms make this possible by automatically collecting, analysing, and reporting radiation doses from imaging tools like CT, PET, SPECT, and fluoroscopy. Using standardised DICOM protocols, these systems eliminate the risk of manual entry errors.
Radiation Dose Tracking Platforms
One example is Qaelum DOSE, which uses a "traffic light" system to compare patient doses against national Diagnostic Reference Levels (DRLs). If a study exceeds regulatory limits, it’s flagged with an orange or red indicator, prompting an immediate investigation. Real-time alerts, sent via email or pop-up notifications, further ensure clinical staff can quickly address any breaches in dose thresholds.
In September 2023, I-MED Radiology Network, which operates 250 clinics across Australia and New Zealand, rolled out the Qaelum DOSE platform across more than 200 imaging systems, including CT, PET, and SPECT machines. Their protocol mandates that any dose outlier undergoes a clinical review within 48 business hours. To go a step further, I-MED has set internal benchmarks that are stricter than national standards, ensuring radiation exposure stays "as low as reasonably achievable" while still delivering quality diagnostic results.
These platforms also maintain patient dose passports, which are detailed records of a patient’s imaging history. They track the number of scans, the time between them, and cumulative radiation exposure across facilities. This data allows clinics to customise imaging protocols and uphold the ALARA principle, balancing safety with diagnostic needs. Advanced analytics further enhance accuracy by calculating Size-Specific Dose Estimates (SSDE) based on actual patient images rather than relying solely on phantom-based metrics like CTDIvol, making dosimetry more precise for different body types.
Identifying and Reviewing High-Dose Cases
In addition to automated alerts, thorough review processes play a key role in optimising radiation doses.
When a high-dose case is flagged, radiologists and technicians document justifications – whether it’s due to a patient’s high BMI, complex diagnostic needs, or challenging positioning. This documentation not only ensures regulatory compliance but also creates a transparent audit trail for further investigations.
The benefits of systematic dose tracking are clear. For example, Chris de Angelo, Director of Imaging Services at Cone Health, highlighted its impact:
"With teamplay, we have been able to identify higher dose outliers on our CT protocols and take actions to reduce the overall exposure by 25%"
. Similarly, Dr Nikolaos Papadakis noted that dose management software helped reduce average patient doses by 10–15% in just three months. By pinpointing inconsistencies in imaging protocols and equipment calibration, these systems make it easier to implement standardised protocols across clinics, promoting consistency and ongoing improvements in patient safety.
Dose Optimisation in New Zealand Facilities
New Zealand’s imaging facilities have embraced advanced dose monitoring alongside national regulations to fine-tune imaging protocols, ensuring patient safety without compromising diagnostic quality.
Strict adherence to national radiation safety regulations is a cornerstone of these efforts. These guidelines enforce the ALARA principle – keeping radiation exposure as low as reasonably achievable while still delivering clear, accurate diagnostic results. This balance of safety and precision is a priority across New Zealand’s healthcare facilities.
Radiologists and Medical Radiation Technologists (MRTs) in New Zealand are specially trained to minimise radiation exposure while maintaining diagnostic accuracy. They carefully tailor imaging techniques to each patient’s size and specific clinical needs. By combining their expertise with advanced imaging technologies, these professionals ensure that only the necessary dose is used to capture the required diagnostic information.
Locating Clinics with Dose-Efficient Imaging
Platforms like Radiology Clinics NZ simplify the process of finding imaging facilities that prioritise dose optimisation. You can filter searches by region – whether you’re in Waikato, Canterbury, Otago, or Wellington – and by specific imaging procedures such as CT, MRI, PET-CT, or digital X-rays.
When browsing clinic profiles, look for terms like "dose efficient", "integrated intelligence", or "leading-edge equipment." For instance, Beyond Radiology highlights its digital radiography systems that use integrated intelligence to cut examination times by 20% or more while reducing radiation exposure. Similarly, Pacific Radiology, with its extensive network of 47 clinics, emphasises its use of advanced equipment designed for dose monitoring and reconstruction. These descriptions reflect how New Zealand’s rigorous safety standards influence the protocols and technologies available at these facilities.
Reviewing Facility Protocols and Patient Services
Clinic profiles on Radiology Clinics NZ often include details about services like electronic access to imaging results through platforms such as "myImaging." These tools can help patients track their imaging history and avoid unnecessary repeat scans. Interestingly, research indicates that 64.12% of patients want to know the exact radiation dose they receive during diagnostic procedures. Before booking an appointment, it’s worth contacting the clinic to confirm whether they provide dose details in their reports and employ low-dose protocols with advanced reconstruction techniques. Patient reviews can also shed light on how well staff communicate safety measures and procedure details.
If there’s any chance of pregnancy, always inform the technologist. This will activate specific safety protocols to further reduce radiation exposure, a standard practice across all New Zealand facilities.
Conclusion
Balancing minimal radiation exposure with accurate diagnostics is a cornerstone of modern medical imaging. The ALARA principle – "As Low As Reasonably Achievable" – guides this balance. As the International Commission on Radiological Protection (ICRP) points out:
"Dose reductions for imaging or x-ray-image-guided procedures should not be used if they degrade image quality to the point where the images are inadequate for the clinical purpose".
This approach ensures that while long-term radiation risks are minimised, diagnostic precision isn’t compromised.
Technological advancements, such as iterative reconstruction algorithms and AI-powered deep learning systems, have revolutionised dose reduction. These innovations can cut radiation exposure by up to 95% in some procedures. Imaging facilities across New Zealand have embraced these tools, aligning them with strict national regulations. Medical Radiation Technologists and radiologists work together to customise imaging protocols for each patient. From fine-tuning scanner settings to leveraging AI-driven reconstruction techniques, every step reflects a commitment to patient safety.
New Zealand facilities also focus on optimised protocols, understanding that radiation exposure accumulates over a lifetime. However, digital imaging systems often adjust images automatically for optimal clarity, regardless of the dose used. This makes it difficult to gauge dose safety based solely on image quality. To address this, resources like Radiology Clinics NZ allow patients to search for clinics by region and find those that prioritise dose-efficient technologies, advanced equipment, and intelligent systems.
Before your next scan, review clinic profiles for mentions of features like iterative reconstruction, AI-based systems, or dose monitoring. You can also contact facilities directly to ask about their protocols and dose reporting practices. Notably, 64.12% of patients express a desire to know their exact radiation exposure. By choosing clinics dedicated to optimising imaging practices, you ensure that each procedure delivers the highest diagnostic value with the lowest possible radiation risk.
FAQs
What radiation dose numbers should I ask for on my CT report?
When discussing your scan, it’s a good idea to ask about the radiation dose specific to your procedure. For instance, a head CT scan usually involves exposure of around 1–2 mSv, whereas an abdominal CT scan typically falls between 8–10 mSv. These figures are often detailed in CT reports, giving you a clearer picture of your exposure levels.
Is deep learning reconstruction safe, and does it miss anything important?
Deep learning reconstruction offers a reliable way to reduce radiation doses in CT imaging while maintaining quality. However, there’s a potential risk of missing critical details if the algorithms aren’t carefully calibrated or thoroughly validated. Researchers are actively working to enhance the precision and consistency of these methods to tackle such challenges.
How can I check if my clinic uses low-dose protocols in New Zealand?
You can talk to your clinic about the imaging technology and protocols they use to keep radiation exposure as low as possible. Ask about their equipment specifications and whether they use low-dose protocols, like Planmeca Ultra Low Dose™, or similar technologies aimed at optimising radiation levels.
Related Blog Posts

Leave a Reply